There has been in the recent months a series of claims
- Not enough evidence of the benefits of telemedicine (TM)
- More random trials are require
- No EBM (evidence based medicine) is shown with telemedicine
- Not enough publications…
And from the publications existing results were negative. After that a long series of replications based on the non-proven benefits or equal health costs or hospital re-admission, at least in heart-disease have been published.
Hopefully some others including ourselves have been pointed out that to carry out TM trials and published and evaluate results one have to be trained in the BoK (Body of knowledge) of telemedicine to understand all the implications and how to compare data (similar no-adhesion or drop up).

Applying the same heuristics to TM trials than those for pharmacology benefit of substances is an error. There are many other benefits that have never been considered in pharma-trials. Let me list some of them in here:
- Patient´s opinions: expenses, confort, lack of stress, support availability, smooth care, individual respect…
- Familiar or care opinions: expenses, confort, lack of stress, support availability, quick response…
- Patient benefits: Integrated care, control of Health-social determinants, Psycho-social factors, QUALY (years of quality of life), RLE (real life evidence), prevent worse-health consequences.
- Healthcare system: W2P (willigness to pay), decrease workload, efficiency, changes on the channel of care, digital supervision, ML (machine learning), Digital supervised medicine.
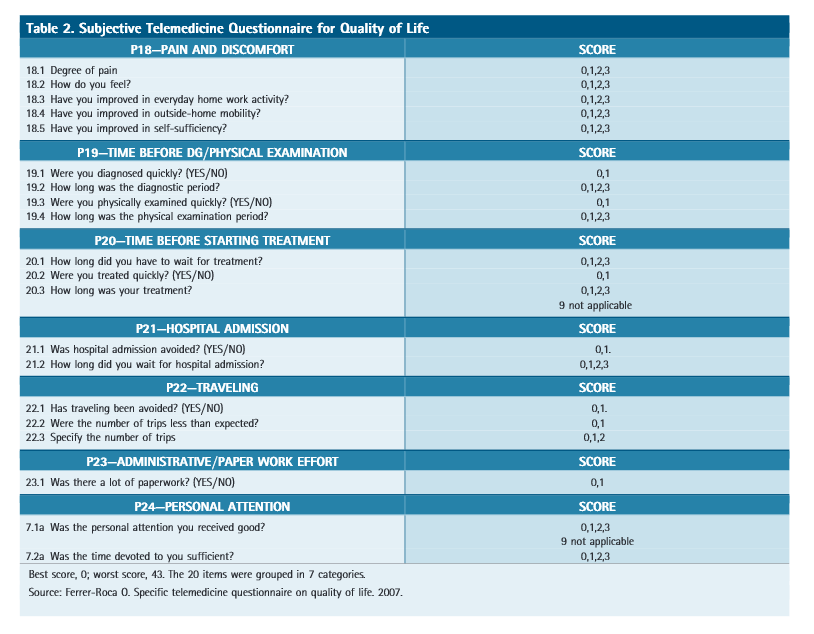
For that reason we designed a Specific TM questionaire for QUAL, 2007, Ferrer-Roca O. allowing to evaluate results from the point of view of the patients: “Telemedicine care by a hospital specialist through videoconferencing was comparable to hospital referral for face-to-face medicine. Teleconsultations managed by nurses had a positive impact on the QoL of rural patients. They did not have to travel and thus diagnoses and examinations to start treatment were initiated faster”
Keep in mind that HEALTH DETERMINANTS are
- 40% Socioeconomic factors.
- 40% Life style.
- 10% Ambient quality.
- just 10% Healthcare system quality.
If we address the three first with Telemedicine and distant care as the one proposed by H2O – Humanization of Healthcare, we improve citizen health and patient health by 90%.
See also: Fracaso de la medicina. Investigacion ciudadana frente EBM.

